
- Current
Dr Donald Lamont C.Eng, FICE, Director, Hyperbaric and Tunnel Safety Ltd of the UK welcomes publication of the article on the use of German decompression tables and adds experiences of using the Blackpool Tables for decompression operations in the UK and comments on other aspects of the data presented in the article.
Read the full text of the Feedback article on the Feedback page or in the Feedback entry at the bottom of the article. Use the Feedback service or send an email to add your thoughts, comments, and experiences to the discussion.
A detailed review of the compressed air working programmes on a series of pressurised TBM projects and compressed air tunnel headings provides the data for publishing the experiences of these intervention and decompression cycles and the influences on the incidences of decompression illness. The data and findings are compiled by Stephan Assenmacher, who has been a general site manager of TBM projects for Hochtief since 1997 and has more than 20 years of experience in compressed air work; and Dr Wolfgang Förster, who is an expert in hyperbaric medicine and Chairman of the Hyperbaric Pressure Working Group at the head office of the statutory accident insurance executive in Germany. He has been associated with many compressed air working projects and both are members of the German Work Group on Guidance for safe working in compressed air.
Working in compressed air was first used for sinking caissons for bridge foundations and for excavating tunnels completely under compressed air conditions. Working in compressed air has since become standard in pressurised TBM tunnelling. As air-only decompression had resulted in several cases of decompression illness in the past, work in compressed air, and the decompression procedures themselves, had to be reassessed. As a result oxygen decompression was implemented into the decompression procedure.
Oxygen decompression is beneficial for a faster exchange of nitrogen, which is dissolved in the bloodstream in the exposed operative. Pure oxygen is administered during decompression via a breathing mask and at pressure levels of 1.0 bar and 0.5 bar. The higher amount of physically dissolved oxygen in the blood serum and body tissues makes for a better outcome after partial nitrogen saturation of the exposed individual worker. Because of the beneficial effect, application of oxygen in compressed air work became the legal standard in the German Verordnung uber Arbeiten in Druckluft (DruckL V) in 1997.
Other countries also implemented oxygen decompression, although most of them do not have their own regulations. In Spain, for example, decompression from compressed air work is controlled by the Ministry for Fishing, which also deals with diving works. In France, the decompression tables allow decompression up to 4.0 bar but oxygen decompression is only used as an option. The Netherlands creates individual decompression tables specific for each project. Poland used the German TBG Tables for recent pressurised TBM projects in Danzig and Warsaw. Decompression operations in Austria, Switzerland, Ireland and Malaysia are also based on the German TBG tables. In the UK, oxygen decompression was implemented in the former Blackpool Tables.
The following report presents a summary of compressed air exposure data collected from several projects – each of them with special particularities – since implementation of oxygen decompression into the TBG Decompression Tables. Data from more than 2,500 individual exposures are compiled, reviewed and evaluated. More than 20% of these exposures took place in a pressure of 1.8 bar and greater. All types of compressed air work are included in the record, including caisson construction, TBM tunnelling and excavation in compressed air.
The following aspects were considered in particular:
The following projects, all using the TBG Decompression Tables, were evaluated:
The evaluation of exposure data was completed only by those who had worked on the project as the person in charge of the compressed air work, or as the appointed medical doctor.
The Herrentunnel in Lübeck is a twin tube road tunnel replacing the old bridge over the River Trave in the city of Lübeck. Both tubes had a length of approximately 790m and were excavated with a slurry TBM of 11.68m bore diameter. The geology was mainly marl, silt and sand, blocky material and glacial boulders. The southbound drive was excavated from December 2002 to April 2003. The northbound drive followed from July 2003 to October 2003.

Shortly after the launch of the southbound drive the TBM had to pass a layer of blocky material and glacial boulders. Several of these boulders were ripped out of the matrix by the cutterhead, and turned within the cutterhead – causing massive damage to the steel structure and the cutter tools. Excavation was suspended for three weeks while repairs requiring cutting and welding work in compressed air were carried out.
Shortly after restart of the excavation, once again boulders were found in the excavation chamber. They had to be crushed by means of hydraulic blasting. Just before passing under the River Trave a boulder was blocking the submerged wall opening. The boulder had to be removed manually and by diving into the bentonite since a full drawdown of slurry in the excavation chamber was not possible in that area. In addition, the grill in the invert behind the stone crusher was damaged and also had to be repaired by divers.
Before and after passing under the River Trave, disc cutters, scraper tools and buckets on the cutterhead had to be replaced.
In total, 785 individual exposures, in a pressure range between 1.8 bar and 3.1 bar, took place during the southbound drive. Sixteen cases of decompression illness (about 2% of individual decompressions) had to be treated. Reasons for this high number are explained below.
From the experience of the first drive, the number of inspections of the cutterhead was increased on the second drive. Shortly before passing under the river, divers were required to remove a boulder found in the submerged wall opening. Some tool changes took place but the number of individual interventions could be decreased to 164 in a pressure range of 2 bar to 3.6 bar with two cases (or 1.2%) of decompression illness treated.
The LRT link to the airport in Hamburg is a twin tube tunnel. Main structures included two deep caissons of up to 40m (Lots 6 and 7) and the twin tube tunnels (Lots 5.1 and 5.2) each about 1750m long and excavated using a 6.9m diameter slurry TBM. The prevailing geology consisted of sands, gravels, silts and marl.

The caissons were sunk from May 2004 to April 2005 with operatives working in compressed air on a regular basis so that there was acclimatisation to that kind of work.
The pressure range was from 0.2 bar to 3.3 bar, increasing slightly as work progressed.

In total 1,068 exposures took place and four cases (0.4%) of decompression illness were treated.
The tunnels were driven from January 2005 to September 2005 (Lot 5.2) with 335 individual compressed air exposures, in a range from 2.8 bar to 3.4 bar, and seven cases of decompression illness (2.1%) were treated. From January 2006 to July 2006, Lot 5.1 was excavated with 219 individual exposures, from 3.2 bar to 3.4 bar, and three cases of decompressions illness were treated (1.4%).
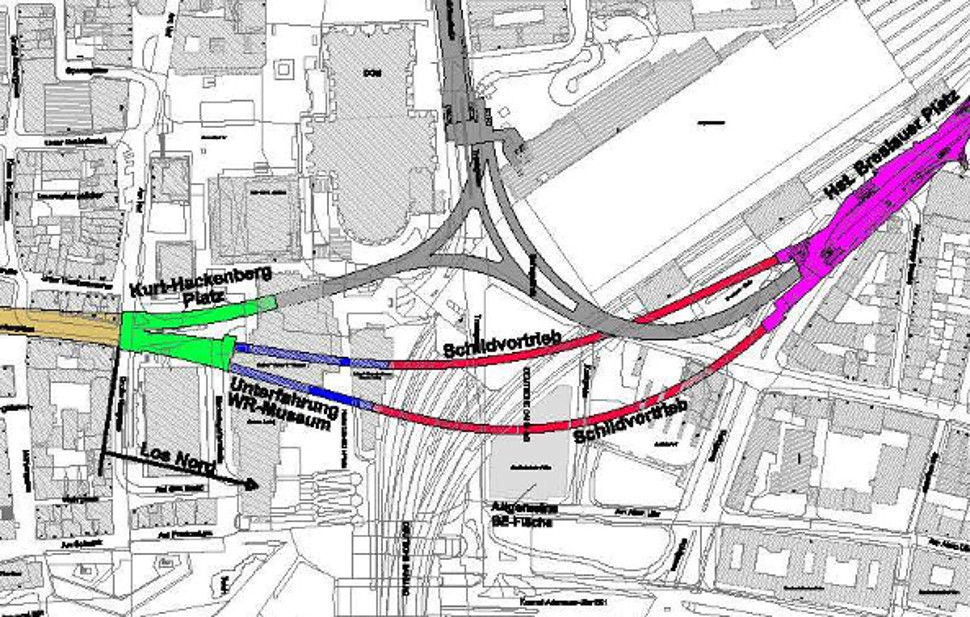
The Metro Cologne Lot North is a short 250m twin tube tunnel under the main railway station of the city. At the end of the two TBM drives a section of about 100m was excavated in compressed air.
The TBM tunnels were excavated using a 6.81m diameter slurry TBM working mainly through sands, gravels and zones of jet grouting and fissure grouting ground improvement.
The eastbound tunnel was excavated from July 2006 to October 2006 and the westbound tunnel from December 2006 to February 2007.
Although only 250m long, repair works were required on the TBM drives to repair damage to the cutterhead caused in one tunnel by blocked disc cutters, and in the other tunnel by an unknown steel sheetpile left in the ground from a former construction project. These repair works included welding in a compressed air environment. In the eastbound tunnel, 180 individual exposures in pressures of 1 bar to 2.1 bar were executed without any cases of decompression illness. For the westbound tunnel, 133 individual exposures were recorded with most of them (84%) at 2.6 bar, and also without any cases of decompression illness.
The compressed air tunnel drive was excavated from the opposite side of the main railway station towards the TBM. A metro had been planned on the alignment and before the new Cologne Philharmony concert hall was built on the surface. Diaphragm walls and a concrete lid structure were installed to allow the metro tunnels to be built at a later stage. Within these diaphragm walls and the roof, the tunnel was excavated using a compressed air environment from June 2007 to February 2009, with operatives working in compressed air on a regular basis. In total 16,350 individual exposures took place in a range between 0.8 bar and 1.8 bar. The number of instances of Type I decompression illness was less than three.
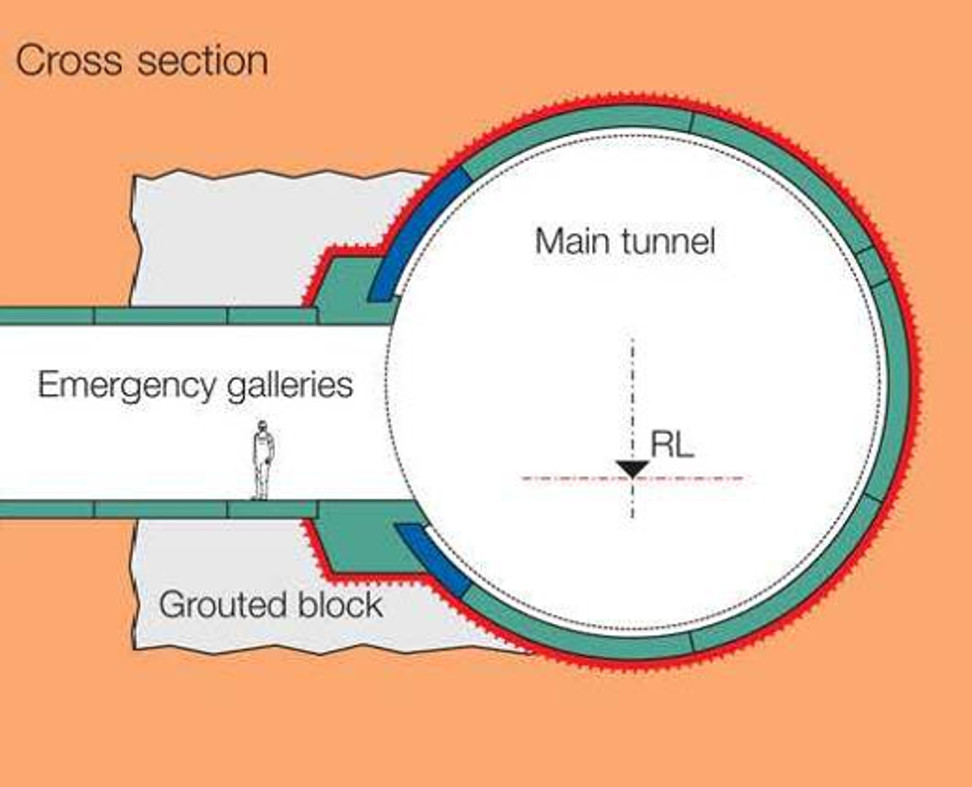
The Jenbach H8 tunnel is part of the new north-south railway connection between Berlin and Milano, through the Inn Valley in Austria. A 3,467m long single-tube double-track tunnel in the valley was excavated using a 13m diameter slurry TBM with a low overburden to an existing surface railway and motorway. The geology consisted mainly of sands, gravels, silts, ground improvement zones of jet grouting and mixed face conditions of rock and soft soil towards the end of the tunnel drive. Emergency evacuation shafts were to be installed at 500m intervals and to the side of the main tunnel. These were connected to the main tunnel using the pipe jacking method with a 4m diameter TBM. The connections into the main tunnel were achieved with hand mining through blocks of ground improvement and working in compressed air.
The main tunnel was excavated from November 2007 to April 2009. Due to high wear on the cutter tools a great number of compressed air interventions had to be executed. Most interventions took place to change worn cutters. Welding repair works were also required on tool fixings. In total, 1,306 individual exposures from a pool of 96 compressed air operatives were completed during the main tunnel drive, working under pressures ranging from 1 bar to 2.8 bar. No cases of decompression illness had to be treated.
Connections of the rescue tunnels to the main tunnel were completed in compressed air conditions during the period July 2008 to March 2009. In total, 2,558 individual exposures from a pool of 120 compressed air operatives were completed. Working pressure varied between 1.9 bar and 2.7 bar, and again no cases of decompression illness occurred.
The XFEL complex for nuclear physics experiments consists of a total 11 tunnel drives of lengths from 137m to approximately 2,000m. The three tunnels of Lot 2 were excavated by a 6.18m diameter slurry TBM while the 8 tunnels of Lot 1 were excavated using a 5.45m diameter slurry TBM. The tunnels are excavated through deposits of mainly sands, gravels, silts and marl.

The tunnels of Lot 2 were excavated from July 2010 to July 2011, and those of Lot 1 were excavated from February 2011 to June 2012.
The compressed air work on both lots can be described as a normal number of cutterhead and face inspections, some single tool changes, one obstacle removal, and cleaning of the pressure release chamber following each breakthrough. In total 225 individual exposures were undertaken on Lot 2, in pressures range from 0.9 bar to 1.4 bar; and 231 exposures on Lot 1 under pressures of 1.2 bar to 2.4 bar. No cases of decompression illness were observed in either Lot 2 or Lot 1.
The Corrib tunnel is built to connect an offshore gas pipeline from the Atlantic Ocean to the onshore gas terminal. The 4,900m long tunnel drive was excavated from 2012 to 2014 using a 4.2m diameter slurry TBM. The geology consisted mainly of highly abrasive sandstone, which resulted in a high number of compressed air interventions for tool changes. Working pressures ranged between 1.3 bar and 2 bar and had to be adjusted to account for the tidal influence of the Atlantic Ocean.
More than 50 compressed air interventions had to be performed with a total of 767 individual exposures and decompression procedures. The health and safety management system for compressed air work was performed according to the German compressed air work regulations Druckluftverordnung (DruckLV).
The typical exposure conditions included strenuous physical work in a confined space situation and in a sultry working climate of high temperature and high humidity. The decompression tables have been adapted to the working conditions by the appointed compressed air medical doctor.
The need of hot works required the performance of additional health and safety procedures, including wearing face masks and hoses to feed unpolluted breathing air from outside the working chamber. All requirements were coordinated with the appointed doctor.
During the construction period one minor case of Type I decompression illness (0.1%) had to be treated in the on-site hyperbaric treatment chamber.
The Isebek sewer in Hamburg is a 23m deep tunnel of 2,400m long in the inner City of Hamburg and is being completed by a 3m diameter pipe jacking TBM. In addition, five caissons will be sunk onto the tunnel as inspection and connection facilities. Working pressures will range between 1.2 bar and 1.7 bar.
A high number of hot works have already been performed to replace worn tools and repair damage to the cutterhead. Following the local health and safety rules, breathable air from outside the working chamber was supplied via hoses and face masks. Following completion of approximately half the tunnel drive, 812 individual exposures with oxygen decompression had been recorded. No compressed air work-related health problems or decompression illness had been reported.
In general, compressed air work has to be seen as potentially very hazardous work. During the design and planning phase of a project that is likely to require compressed air work, consideration should be given to the environment in which that work will have to be executed.
Several aspects affect the compressed air operative while working in compressed air. The effect on each individual might be different within the intervention team. It can also be different for the same individual from one intervention shift to the next, depending on his general health at any particular time.
Psychological aspects also play an important role in compressed air work. Not everyone deemed fit to carry out compressed air work by the annual medical examination, is also fit from a psychological point of view. A first indicator is the trial pressurisation that will be carried out once the operative has successfully passed his medical appointment. The operative will be accompanied by an experienced compressed air operative who observes his charge during the trial. In most cases the trial pressurisation is only carried out up to 1 bar to determine if the new operative is able to achieve pressure equalisation and whether he shows any symptoms of agoraphobia. For familiarisation reasons, and also for observation of his behaviour in higher pressure stages, where nitrogen narcosis might occur, it should be assessed whether the operative in question should be pressurised up to the stage where he will later work.

Nevertheless, trial pressurisation in a medical chamber is different from work in real compressed air situations, and decompression in the man lock thereafter. The severe environment of a confined space, which the operative knows he can only leave upon completion of a time-consuming decompression procedure, together with other severities such as noise, humidity, heat or cold, or air quality, might be aspects that an operative is fearful of, or at least feels such a discomfort level in such conditions that he must to be classified as not fit for compressed air work.
These symptoms should be recognised by an experienced compressed air contractor, person in charge, or hyperbaric supervisor, even if the affected operative does not voice his concerns. No one should be forced to work in compressed air, even if they are physically fit. Compressed air work must be absolutely voluntary.
In addition to geometrical restrictions, and psychological aspects, the severity of the work itself affects the health of the compressed air worker. There is a great difference between the compressed air operative completing an intervention to inspect the cutter tools of a TBM, or to assess the geological situation at the face, and interventions in which physical work such as tool changes, obstacle removal, repair work, cleaning work or cutting and welding work are required.

The basic health impact in compressed air work is caused by nitrogen saturation of human tissue. The level of saturation is dependent upon the actual tissue perfusion, which again is dependent upon the operative’s breathing and heart rate. Taking into account the stress and strain of physical work is mandatory to avoid supersaturation of tissue before decompression starts.
Manual handling should be simplified by use of special devices such as a device for the assembly of cutter discs on a TBM cutterhead for example. Lifting eyes should be installed in several locations to allow various possibilities for fixing chain hoists to facilitate the moving heavy items into position.
Avoiding forced postures such as kneeling during execution of the works has to be considered, as well as impediments caused by having to use additional respiratory equipment to complete cutting and welding operations in a compressed air environment.
Acclimatisation to compressed air work is another key factor. In the case of a caisson or a tunnel that is excavated within a compressed air environment, the operatives will regularly be subjected to that working environment. They are acclimatised to compressed air work. Pressure levels will increase slowly with the performance of the works. On TBMs, compressed air work is normally periodic, occurring only in cases where inspections or tool changes are required. This has to be taken into account in addition to the pressure levels at which the works will be executed.
Tunnelling requires working in confined spaces. Access and egress from the tunnel are restricted during construction to only one direction. Compressed air work has to be seen as an additional confined space work within an already-existing confined space. Access and egress are restricted through the man lock into the compressed air chamber, and from the pressurised environment back to atmosphere.
In addition, the work area for the compressed air operative is different depending on the size of the excavation chamber of a TBM, of the working chamber of a caisson, or of a tunnel being excavated completely in compressed air.
On slurry TBMs it has to be considered that in most cases a half drawdown of the slurry is sufficient for the work that has to be executed in compressed air. A full drawdown of the slurry will be avoided as far as is reasonably practicable and only be considered if there is the need to work in the lower part of the TBM – such as for repair of the stone crusher. On larger diameter TBMs there might be the need to drawdown by only a third if the support pressure calculation does not allow for a half drawdown. On the one hand the drawdown of slurry should occur as little as possible to maintain pressurised support of the face and minimise the risk of a blow out. On the other hand this means further limitation of an already narrow space in the working and excavation chamber.
On caissons the access from the working chamber to the man lock might be restricted if it is a deep caisson with a shaft pipe and ladder or man hoist.

The bore diameter of a TBM and the diameter of the main bearing are integral to the size of the installed man lock. On smaller TBMs, in most cases, a single man lock can be installed within the shield body. According to the requirements of EN12110 the height of the man lock has to be at least 1.8m. It consists of a pre chamber and a main chamber, with the two locks positioned either in-line or next to each other. The space inside the locks is very limited because there are other installations within the lock, including oxygen breathing systems, water sprinklers and lighting.
On TBMs of more than 9m diameter, there may be an opportunity to install a double lock system, with each system comprising a pre chamber and a main chamber.
Feeling comfortable inside the man lock during decompression is an essential contributory factor for the health of the compressed air operative. Long decompression times, in combination with the need to wear oxygen masks and restricted possibilities to move the main joints such as elbows and knees, all contribute to cases of possible decompression illness.
Measures should already be foreseen in the planning phase of a project to avoid, as far as is reasonable, the need for compressed air work activities. Possible solutions could be the installation of wear detection systems on the cutterhead and cutter tools, or identifying areas where interventions to the cutterhead might be carried out at atmospheric pressure such as in pre-installed grout blocks or intermediate shafts.
Where compressed air work cannot be avoided, the design of the locks and chambers themselves should allow for an ergonomic decompression procedure. Regular short inspections of the chambers should be carried out to avoid the need for heavy repair work later, caused perhaps by a poor maintenance regime. A sufficient number of compressed air operatives should be foreseen to execute compressed air work.
The working times that are listed in the decompression tables do not take into account all adverse factors explained in the preceding chapters. The working time therefore has to be seen as the maximum allowable time, a limit that must be decreased following consideration of all adverse circumstances of the planned intervention. It shall be reduced in a way that the health of the compressed air worker can be ensured. Additionally, breaks should be offered to the compressed air operative depending upon the severity of the work being executed.
The correct behaviour of the compressed air operative is also essential to avoid cases of decompression illness. There are certain rules and guidance for the compressed air operative, as follows:

In total, more than 25,000 individual exposures across the sever projects in the study have been evaluated. In total 36 cases of decompression illness Type I occurred (a 0.14% incidence rate) (Table 2). Of these, 32 cases occurred on projects prior to 2006, during which time there were 2,600 individual exposures (a 1.24% decompression illness Type I incidence rate). For the 22,400 individual exposures recorded during the post-2006 projects there were only four cases of decompression illness Type I (0.02%). For all cases, two reasons for the occurrence of decompression illness can be identified:

The cases of decompression illness that still occurred following more flexible use of the tables were caused by the incorrect behaviour of the operatives themselves. This incorrect behaviour was not intentional. After completing challenging physical work such as tool changeouts, operatives are tired and must sit for long period of time in the man lock. They cannot communicate due to the masks they are wearing and fall asleep with the result that they do not breathe sufficient oxygen. They also do not move their joints during decompression and in some cases they even lean on cold surfaces. This all makes decompression illness more likely after decompression.
Adding to the decompression discussion
Dr Donald Lamont C.Eng, FICE, Director, Hyperbaric and Tunnel Safety Ltd, UK
I very much welcome the article by Assenmacher and Förster on the use of German decompression tables. Whilst the decompression outcome on individual contracts can sometimes be found in the literature, there is little published information on national experience. It is particularly interesting having the authors’ views on the practical issues surrounding compressed air working in accordance with German practice and to realise how similar their experience has been in many ways to my UK experience.
As the authors note, oxygen decompression has become mandatory in many European countries over the past two decades. Although the UK Blackpool Tables with oxygen is the approved decompression regime in the UK, most of what little compressed air work has been undertaken in the last 15 years in the UK, has been done using variants of the German tables. Contractors prefer the shorter more aggressive decompression to the longer slower decompression of the Blackpool Tables. The UK HSE (Health and Safety Executive) Research Report RR126 found that, of the European oxygen decompression tables modelled, no one table was best or worst overall.
With one or two exceptions, the decompression outcomes reported from the use of German oxygen tables appear generally good, for which the authors should be congratulated.
The results for the Lübeck Tunnel, at a decompression illness incidence of around 2%, in the pressure range 1.8 to 3.1 bar, is consistent with UK figures for the Blackpool Tables without oxygen.
In reviewing the factors that appear to affect decompression outcomes, the authors mention the problems of lack of working space. In the days of hand tunnelling in compressed air, with many weeks of man exposures, the manlocks were often fairly large and relatively spacious, particularly if they were combined man-material locks. The men could walk around during decompression. Although seating was often provided, it was usually fairly spartan or rudimentary. Now, with TBM locks, there is a lack of space in the manlocks leading to poor posture and inability to move or even to stretch the legs. As a member of the CEN/TC151/Working Group 4 committee responsible for drafting European standard EN 12110 on Airlocks – safety, we committee members were certainly acutely aware of the need to balance the space requirements of those being decompressed, with the space constraints in modern TBMs.
The problem of posture, which the authors identify, is also familiar. This was not restricted to TBM airlocks. Comments in the lock attendant’s register to report that an operative “fell asleep with arm against chamber wall” were not uncommon against entries recording Type 1 decompression illness in a miner’s arm.
I also recognise the issue of forced posture, especially kneeling, leading to decompression illness events. The problem, in my experience, seemed to occur particularly with fitters and electricians when major failures of pumps and motors occurred, leading to urgent extended maintenance work. I routinely met with the contract medical adviser at the end of a contract to go through the compressed air working data and try to find reasons for decompression illness events.
On the issue of acclimatisation, I have changed my opinion over the years. The pattern of compressed air working has changed with the increased use of TBMs. We have moved from daily exposures for months on end, to intermittent exposures which can be on a weekly or even monthly basis.
Acclimatisation was described by Paton and Walder in their 1954 paper(1). They observed the same group of miners over a period of days, from the start of a contract, and noticed that the daily incidence of decompression illness reduced over time. They considered that observation to be evidence of acclimatisation. In my analysis of UK decompression illness records, I observed a similar effect in groups of miners who had all experienced multiple decompress illness events on UK contracts between 1984 and 2001. However, if acclimatisation exists, then the effect should be demonstrable in both groups and individuals. I postulated that the effect of acclimatisation on individuals should mean that, for persons with multiple decompression illness hits on the same contract, it would be possible to demonstrate longer intervals between successive decompression illness events. I looked at the individual miners on the assumption that acclimatisation would make them less susceptible to decompression illness, and hence increase the time between subsequent decompression illness events, and could find no evidence to support my hypothesis that individuals could become acclimatised.
Of particular interest is the conclusion by the authors that a major reason for a change in the incidence of decompression illness in 2006 was the more flexible application of the tables. The ad-hoc introduction on site of “factors”, has been a feature of decompression procedures in tunnelling for many decades but often went unreported. The ‘one table higher and/or one pressure increment longer’ approach has been used, effectively, as a way of making up for deficiencies in the tables, leading to more acceptable decompression illness incidents. Being aware of such adjustments is very important when analysing or comparing the effectiveness of different tables.
Although the authors, in their symptoms and findings, mention incorrect behaviour by the workers, I wonder whether we should accept that their behaviour is not ‘incorrect’ but ‘normal’ and make adjustments accordingly in the tables.
In looking at the authors’ conclusions, I recognise and agree with most of them, however I wonder if ‘adaptations’ and ‘time surcharges’ is the way forward, or whether more conservative tables are required which take better account of deficiencies in the behaviour of the humans involved. After all, we now have the mathematical modelling capability to predict the likely outcome from any given decompression profile, and, with the use of post-decompression monitoring, we are able to link outcome with prediction and hence reduce the risk of decompression illness in the workforce.
Dr Donald Lamont C.Eng, FICE
Director, Hyperbaric and Tunnel Safety Ltd, UK
1. Paton W.D.M. and Walder D.N. (1954) Compressed Air Illness An Investigation during the Construction of the Tyne Tunnel 1948-50, Special Report Series No 281, London, Medical Research Council
Donald Lamont is a member of the CEN/TC151/Working Group 4 committee responsible for drafting European standard EN 12110 on Airlocks – safety. He is a member of the Compressed Air Working Group of the British Tunnelling Society (BTS) and is Animateur of the ITA Working Group 5 on Health and Safety in Works. As a member of both, Lamont led the publication of the joint BTS/ITA Compressed Air Working Group Guidelines for good working practice in high pressure compressed air ![]()
|
|
|
|
|
